Breast reconstruction surgery
Breast reconstruction surgery is an option for women who undergo a mastectomy. The reconstruction procedure may be performed immediately after the mastectomy (during the same surgical session) or at a later date. For instance, a woman may choose to postpone her breast reconstruction until after she completes her cancer treatment, which may include chemotherapy and/or radiation therapy in addition to surgery.
 The types of breast cancer reconstruction surgery include:
The types of breast cancer reconstruction surgery include:
Tissue expander
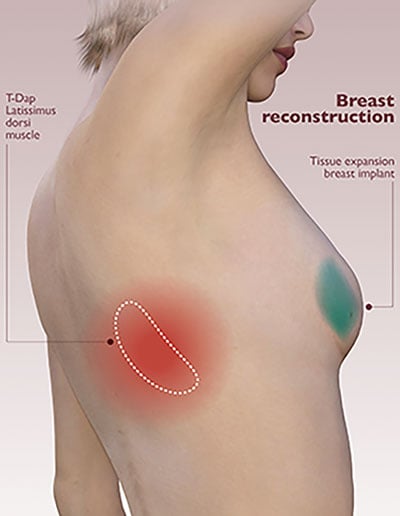
After the breast is surgically removed, a plastic surgeon will place a tissue expander (a special medical device similar to a deflated balloon) underneath the chest wall muscles. Once a week, a member of the patient’s treatment team will add saline solution to the expander to gradually stretch the chest muscles and skin to accommodate the patient’s desired breast size. The “filling” process can take up to six months to complete. At that point, the expander will be replaced with a breast implant.
Latissimus dorsi flap
A latissimus dorsi flap may be a good option for a patient who had radiation therapy or failed flap surgery. During the breast reconstruction procedure, a plastic surgeon will move a portion of the back muscle and skin to the chest to create a new breast. The surgeon may also place a tissue expander underneath the chest wall muscles, which will be gradually filled with saline solution over a few months. Once the patient’s desired breast size is achieved, the expander will be replaced with an implant.
Abdominal tissue flap
During an abdominal tissue flap breast reconstruction, a plastic surgeon moves tissue from the abdomen to the chest to create a new breast. This procedure may be a good option for a patient who has excess abdominal tissue, does not want an implant or would like her reconstructed breast to closely match her natural breast.
There are three types of abdominal tissue flap breast reconstruction:
Traverse rectus abdominal muscle (TRAM) pedicle flap
To construct the breast mound, a plastic surgeon uses a portion of the rectus abdominal muscle along with skin, fat and blood vessels from the lower tummy wall. The surgeon then creates a pedicle, leaving the tissues attached to their base in the abdomen and tunneling them under the skin to the chest.
Deep inferior epigastric artery perforator (DIEP) flap
This type of breast reconstruction surgery is similar to a TRAM pedicle flap procedure in that it uses skin, fat and blood vessels from the lower tummy wall. However, the abdominal muscles are left intact. With the aid of a special microscope, the surgeon performs microvascular surgery to attach the abdominal blood vessels to the chest wall blood vessels.
Muscle-sparing free TRAM
This type of breast reconstruction surgery is similar to a DIEP flap procedure. However, a small piece of muscle (approximately the size of a postage stamp) is taken from the abdomen in addition to the skin, fat and blood vessels needed to construct the breast. Also, instead of being tunneled under the skin from the lower tummy wall to the chest wall, the tissues are completely removed from the abdomen.
Thigh flap
To form the new breast, a surgeon moves skin, fat and blood vessels from the upper inner thigh or back of the thigh. Thigh flap breast reconstruction may be a good option for a patient who is very thin, had a tummy tuck, had a failed TRAM or DIEP flap procedure or prefers not to use abdominal tissues.
There are two types of thigh flap breast reconstruction:
Transverse upper gracilis (TUG) flap
During TUG flap breast reconstruction surgery, a surgeon uses skin, fat and a portion of the gracilis muscle from the inner thigh to create the new breast. Because the gracilis muscle is not a primary leg muscle, there is no loss of function in the leg and minimal risk of hernia development at the donor site.
Profunda artery perforator (PAP) flap
In addition to skin and fat from the inner thigh, a surgeon uses blood vessels that run through the adductor magnus muscle. Due to the location of the donor site, the scar can be well hidden in the groin or lower buttock crease.
If you would like to learn more about breast cancer reconstruction, you are welcome to talk with an expert in the Don & Erika Wallace Comprehensive Breast Program at Moffitt Cancer Center. To request an appointment, call 1-888-663-3488 or complete our new patient registration form online. Our team will also be pleased to help you determine if you are a candidate for oncoplastic breast-conserving surgery, which involves maintaining natural breast contour while resecting a tumor.